![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]() THE TORTOISE
TRUST HOSPITAL: A BRIEF HISTORY
THE TORTOISE
TRUST HOSPITAL: A BRIEF HISTORY
This article first appeared in our Millenium issue newsletter
Jill Martin

Jill Martin of the Tortoise Trust hospital
As this hospital report is the first of this new century, it seemed appropriate to present an over-view of some of the milestones which have taken place in our treatment of sick tortoises over the last 15 years. It has largely been a valuable learning experience for ourselves, our vets and members alike, and it has only been by observing and treating the hundreds of animals that have passed through our doors, that we are now able to advise all interested parties on an extensive range of tortoise-related topics.
During the mid-1980ĺs, the majority of tortoises received at the hospital had suffered frost damage in hibernation. At our small facility in Norfolk over about a three year period, we had dozens that had suffered varying degrees of eye damage, some with accompanying secondary problems such as pneumonia and liver damage.

Cesar - THE first tortoise in the history of the Tortoise Trust!
The vast majority needed daily force-feeding. Some were totally blind having presumably suffered optic nerve damage. Others having suffered lens or retinal damage had partial sight. An early hospital report records the story of Ursula, our first -ever sight-damaged patient:
ôIn May 1985 we received a phone call from an owner whose tortoise was experiencing difficulties emerging from hibernation. We went to investigate and found the poor animal in a truly shocking state. So dehydrated and thin that she felt like an empty shell, jaundiced and eyes tightly shut, it was obvious that without emergency treatment she would very soon be dead. As the owners clearly wanted to see the back of her, they were happy to let us take her into our care. Thus we were faced with our first very poorly patient and the monumental task of trying to salvage what little life there was left in her. It transpired that her poor condition was due to her having been frozen during two consecutive winters. During the interceding summer, Ursula had spent a miserable time tethered by a hole in her shell, blind and unable to feed. The second freeze had brought this already debilitated animal close to death. Her treatment was intensive for many months and we were despondent about her at times as she would not move. However, during the second summer with us, she one day decided to get up and walk, very slowly and shakily at first, but at least it was the start of a new phase in her progress. Two years later she was diagnosed as having perfect eyes, her problems being likely due to optic nerve or brain damage.ö
Ursulaĺs initial treatment was largely experimental, and she received copious doses of concoctions of water, vitamins and Colovet (an iron solution), as well as tubes of baby food. Fortunately, it worked! After this point as other patients flooded in our vet advised the use of Hartmannĺs solution by tube until the kidneys are functioning, followed by a rehydration solution, then on to a liquid feed, at that time Duphalyte which is excellent and still available. We have always stuck to this regime with a severely dehydrated tortoise the only difference being that there are now other liquid feeds available such as Reanimyl and Pronto Joule, the latter being used very recently to great effect, on a sick T. kleinmanni.
In the autumn of 1986 the handbook ôSafer Hibernation and Your Tortoiseö was written by Andy Highfield, in order to educate owners about the correct way to manage hibernation and prevent tragedies from taking place. We believe this book has saved innumerable lives, and tens of thousands of copies have been given away free.

Ruptured ear abscess - box turtle
One common condition that we have always seen is the ear abscess. Back in the 1980ĺs it was usual for the cheesy matter in the ear to be surgically excised, and then for the scale to be sutured. However recurrences were common, as it is rare to be able to remove all the infected matter at the first go. From 1990, our new vet had a different technique where the incision was kept open so that the ear could receive a daily flushing and continual application of a topical antibiotic cream. When the ear is finally clean and heals, recurrence is far less likely.

A bad case of stomatitis (Mouth Rot): one of many such cases
A very useful antibiotic from the 1980ĺs was the Framycetin Anti-scour paste made by C Vet. Coming in a syringe applicator, it was easy to get into an open ear or an infected sore mouth. Unfortunately it was withdrawn from the market in the early 1990ĺs. However we have had equally good results using the cowĺs udder treatments, again in syringes, called Leo Yellow and Leo Red.

A rare photo of our old hospital units, circa 1985
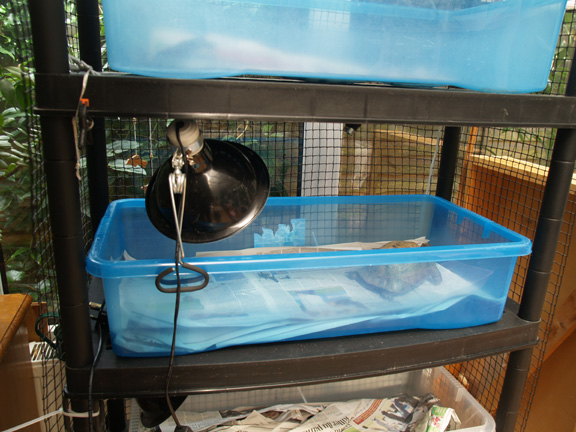
Accommodation-wise, before 1991 we had been using the closed-box type vivarium with sliding perspex doors heated by means of a spot light and under-floor tubular heater. However we became very unhappy about the lack of air-flow under these conditions and noticed that tortoises in such units often developed runny noses and dry eyes. We therefore changed to small wooden sided open-topped pens with plywood bottoms covered in floor tiles. We still usedthese units today in the hospital. They can be easily heated with a clip-on spot light and if necessary, a heat mat underneath. More recently, we changed over to PLASTIC trays based on the same concept. With these, each 'shelf' has two trays, one in use, the other out of use being cleaned. We change them over every day. This is fast, efficient and works very well!
Another area of concern has always been the high incidence of hatchlings and juveniles developing bladder stones. Again this seems to be a problem related to their accommodation. Tortoise babies kept on hard surfaces, even if they are fed correctly and offered water, are prone to developing stones. However babies given a thick natural earth-based medium to bury into are far less likely to develop the condition as their bodies will lose less moisture. We now always recommend this method of husbandry.
Around the year 1988 we began to be
increasingly concerned about the numbers of reports of cases of RNS, gut
parasites, liver disease and mouth rot, in large mixed collections, including
our own. By 1990 we observed that the
tortoises mainly affected by such symptoms were of North African origin, whilst
the Turkish T. ibera were mainly unaffected, as were the Hermannĺs
tortoises. In the summer of 1990 Andy
Highfield attended an international chelonian conference in
In the autumn of 1990 we published a stark warning to all tortoise keepers in a paper entitled ôIs there a Tortoise AIDS in our midst?ö From our own tortoise collection we noted that ôthe first case subject to study was of north African origin and had a history of repeated flagellate attacks, RNS and generalised debilitation; in other words it fitted the clinical profile we are now beginning to recognise as suggestive of chelonian immune suppression syndrome. This tortoise failed to respond to treatment and finally died from pneumonia and liver failure. Immediately after death the liver was removed and subjected to histopathology. The report confirmed our worst fears; ôa large number of the nuclei within the liver cells have a very dense appearance, much different to the other nuclei and this is abnormalö. In all probability ôthese are viral inclusion bodiesö.
We still believe that the most likely
silent carriers of viral disease are the T.ibera which were imported in large
numbers from
By 1993 we still had a number of tortoises who had not been exposed to those suffering from viral problems, but who were still plagued by chronic RNS and pneumonia. However help for these came in the form of the drug Baytril, designed to cope with mycoplasma organisms as well as bacteria. One such tortoise was Beatrice, who still thrives to this day. In a 1993 report we wrote:
ôthis gentle North African tortoise who had been ill for several years with respiratory problems was one of the animals treated this season with the new drug Baytril. Beatrice developed the first signs of RNS five years ago, and despite treatment with various antibiotics, the condition never really cleared up. Twelve months ago she developed pneumonia coupled with jaundice and although these severe symptoms were brought under control, she still suffered from persistent rhinitis and general debilitation. More recently she developed an inability to co-ordinate leg movements, was very jumpy and refused to come out of her shell. She was treated with a twice-weekly vitamin B capsule whereupon the neurological symptoms gradually receded, and at the same time she started on a course of Baytril injections, dosed at 2.5mg per kilo, given at 48 hourly intervals. Within 10 days she had become a new tortoise. Her eyes were no longer sunken, her nose had dried and she was obviously able to enjoy life again.ö
The dose rate tried with Beatrice was actually very low. We now dose at 10mg per kilo.
Baytril has helped innumerable tortoises since the mid 1990ĺs and is still a first choice in the treatment of many conditions. Where there has been some resistance we have had excellent results more recently, with Marbocyl (marbofloxacin) which we now highly recommend.
By the summer of 1994 we had moved to our
new site in

More sheep than people! In 1994 we relocated our facility to rural Wales
In September 1995 our new facilities were
put under pressure by the first influx of sick tortoises from a huge customĺs
seizure in

One of the rescued Libyan tortoises from 1995
However worse was to come. The winter 1995 newsletter carried the
following report: ô Two weeks after the arrival of the small Tunisian
tortoises, we received a call from Customs officers at Heathrow where a
consignment of 72 adult tortoises from
And so began the long job of rehabilitating and rehoming this large number of frail tortoises. We are obviously heavily reliant on members to offer good homes to such animals, bearing in mind that they will need a lot of rather specialised care, extra heat etc. To this day we still have some old ladies for whom homes have not been forthcoming.

Jill works with a large Algerian female
Since the coming of the Libyans, we have received many other customĺs seizures, including Leopard tortoises, Moroccan T. graeca, T. klienmanni, Tunisian tortoises, Red Eared terrapins, Leopard tortoises and Horsfieldĺs tortoises. We hope to help yet more in the future, and we have no doubt that the experiences of the last 15 years will continue to be drawn upon in our work to come.
(c) 2000-2002 Tortoise Trust